Istanbul · Male Rhinoplasty
Masculine profile preserved, refined.
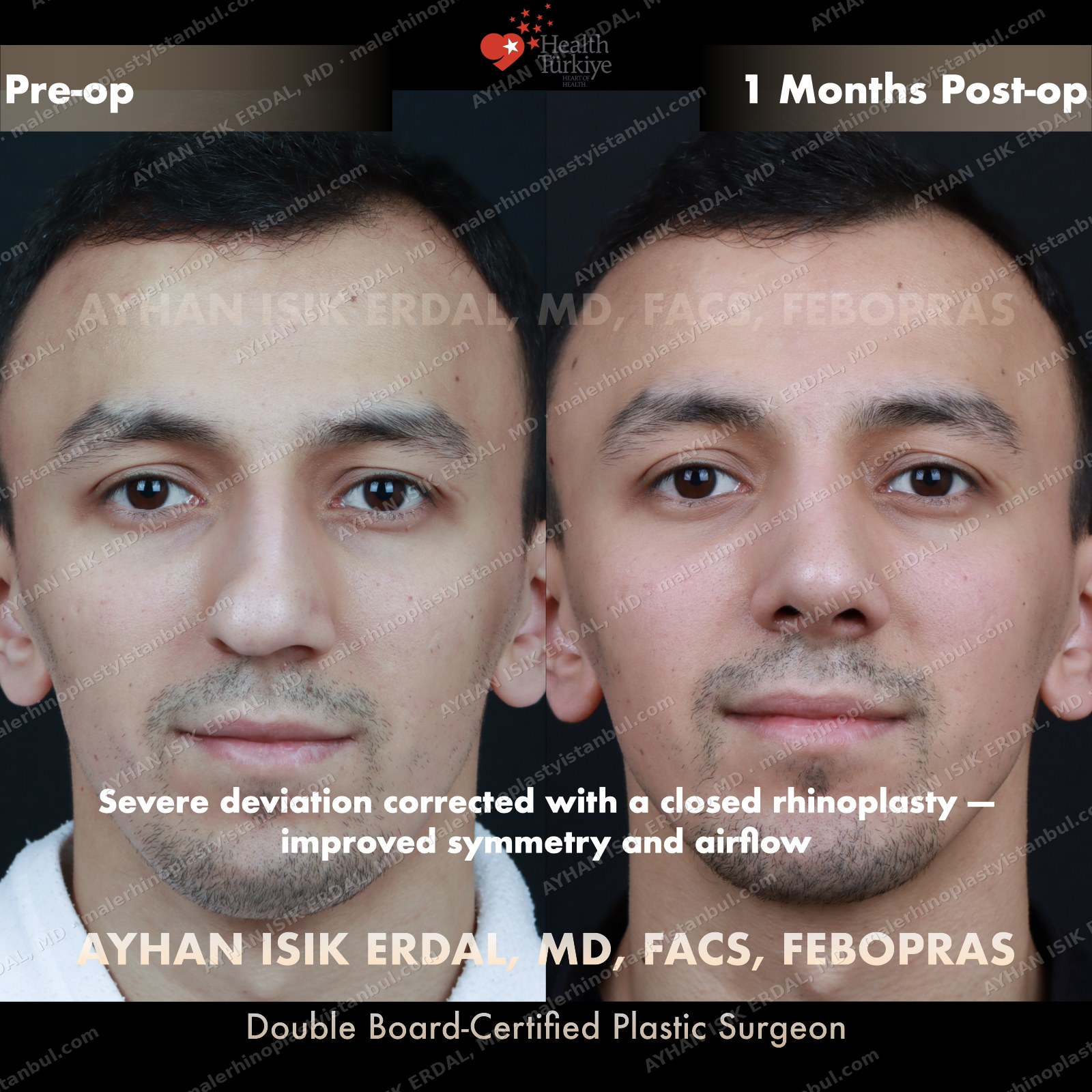
Male rhinoplasty is not female rhinoplasty performed on a man. The aesthetic targets are different: a straight dorsum rather than a gentle curve, a 90–95° nasolabial angle rather than the feminine 100–110°, stronger tip projection, and — above all — no feminisation. Dr. Erdal's approach begins with preserving masculine identity and refines from there.

Fellow · FACS
American College of Surgeons · 2025